
服务热线:0538-8161816


添加日期:2025年01月01日

周全,高延征,吕东波,张敬乙,陈书连,曹臣*
(河南省人民医院/郑州大学人民医院脊柱脊髓外科, 河南郑州 450003)
摘要:[目的] 比较单侧双通道内镜下髓核摘除术(unilateral biportal endoscopic discectomy, UBED) 与经皮椎间孔内镜椎间 盘切除术(percutaneous transforaminalendoscopic discectomy, PTED) 治疗单节段腰椎间盘突出症的临床疗效。[方法] 回顾性分 析 2021 年 1 月—2021 年 12 月应用内镜手术治疗的单节段腰椎间盘突出症 118 患者 。依据术前医患沟通 ,58 例采用 UBED, 另外 60 例采用 PTED。 比较两组围手术期 、随访和影像资料。[结果] 两组患者均顺利完成手术 ,UBED 组在术中透视次数 [(1.4±0.5) 次 vs (7.4±1.5) 次, P<0.001] 显著少于 PTED 组 ,但两组手术时间 [(60.6±0.9) min vs (62.0±9.4) min, P=0.470]、下床行走时 间 [(1.7±0.5) d vs (1.6±0.6) d, P=0.705] 及住院时间 [(4.4±1.0) d vs (4.4±0.9) d, P=0.862] 差异均无统计学意义 ,但是 ,UBED 组治疗 费 [(30.5±0.8) 千元 vs (26.4±1.6) 千元, P<0.001] 显著高于 PTED 组 。随时间推移 ,两组腰腿痛 VAS 评分及 ODI 均显 著改 善( P< 0.05); 相应时间点 ,两组间腰腿痛 VAS 评分及 ODI 评分的差异均无统计学意义( P>0.05)。 影像方面 ,与术前相比 ,末次随访 时两组椎管占位面积率均显著下降( P<0.05), 而椎间隙高度和腰椎前凸角无显著变化( P>0.05)[结论] UBED 治疗单节段腰 椎间盘突出症临床疗效与 PTED 相似 ,虽然 UBED 透视辐射更少 ,但住院花费相对更多。
关键词:腰椎间盘突出症 ,单侧双通道内镜椎间盘切除 ,经皮椎间孔内镜椎间盘切除
中图分类号:R681.53 文献标志码:A 文章编号:1005-8478(2024)24-2228-06
Unilateral biportal endoscopic discectomy versus percutaneous transforaminal endoscopic discectomy // ZHOU Quan, GAO Yan-zheng, LÜ Dong-bo, ZHANG Jing-yi, CHEN Shu-lian, CAO Chen. Department of Surgery of Spine and Spinal Cord, Henan Provincial People's Hospital, Zhengzhou University People's Hospital, Zhengzhou 450003, Henan, China
Abstract: [Objective] To compare the clinical consequence of unilateral biportal endoscopic discectomy (UBED) and percutaneous transforaminal endoscopic discectomy (PTED) in the treatment of single-segment lumbar disc herniation. [Methods] A retrospective re⁃ search was done on 118 patients who had single-segment lumbar disc herniation treated by endoscopic surgery from January 2021 to De⁃ cember 2021. According to preoperative doctor-patient communication, 58 patients were treated with UBED, while other 60 patients were with PTED. The perioperative, follow-up and imaging data of the two groups were compared. [Results] All patients in both groups had oper⁃ ation performed successfully. Although the UBED group had significantly less intraoperative fluoroscopy times [(1.4±0.5) vs (7.4±1.5), P< 0.001] than the PTED group, there were no significant differences between the two groups in terms of operation time [(60.6 ± 0.9) min vs (62.0±9.4) min, P=0.470], bed rest time [(1.7±0.5) days vs (1.6±0.6) days, P=0.705] and hospital stay [(4.4±1.0) days vs (4.4±0.9) days, P= 0.862]. However, the UBED group consumed significantly higher medical cost than the PTED group [(30.5±0.8) k-yuan vs (26.4±1.6) k-yu⁃ an, P<0.001]. As time went on, the VAS and ODI scores in both groups were significantly improved (P<0.05), which proved not significant⁃ ly different between the two groups at any corresponding time points (P>0.05). Regarding imaging, the spinal canal occupied area ratio de⁃ creased significantly in both groups at the last follow-up compared with that preoperatively (P<0.05), while the intervertebral space height and lumbar lordotic angle remained unchanged significantly (P>0.05). [Conclusion] UBED achieves comparable clinical outcometo PTED in the treatment of single-segment lumbar disc herniation, although UBED has less fluoroscopic radiation, while more hospitalization costs over the PTED.
Key words: lumbar disc herniation, unilateral biportal endoscopic discectomy, percutaneous transforaminalendoscopic discectomy
腰椎间盘突出症(lumbar disc herniation, LDH) 是引起腰痛、下肢放射性疼痛及麻木、无力的常见脊柱外科疾病 ,严重者可导致马尾神经功能障碍。腰椎 间盘突出症的一线治疗是非手术治疗 ,包括物理治 疗、药物治疗和硬膜外类固醇注射等 ,而手术较保守 治疗可更快地缓解症状[1,2]。传统的代表性手术是椎 板开窗髓核摘除术 ,但传统开放手术有创伤大、肌肉 牵拉时间长、椎体不稳等可能并发症[3]。随着医疗微 创技术不断进步 , 经皮椎间孔内镜椎间盘切除术 (percutaneous transforaminalendoscopic discectomy, PT⁃ ED)用于治疗腰椎间盘突出症并取得了良好临床效 果 [4~6]。 近 年 来 , 单 侧 双 通 道 内 镜 下 髓 核 摘 除 术 (unilateral biportal endoscopic discectomy, UBED)技术 为微创内镜下治疗 LDH 等腰椎退行性疾病提供了一 种新的选择[7~9]。本研究对 2021 年 1~12 月于本院脊 柱外科行 UBED 患者 58 例与 PTED 的患者 60 例进行 回顾性分析 , 比较两种手术的临床疗效及优缺点。
1 资料与方法
1.1 纳入与排除标准
纳入标准:( 1) 符合 LDH 诊断标准 ,症状 、体 征集中于单侧下肢 , 可伴急性腰背痛;(2) CT 或 MRI 主要阳性表现为单节段 、单侧硬膜囊和神经根 受压;(3) 病程超过 6 周 , 系统保守治疗无效 ; (4) 随访时间 12 个月以上。
排除标准:( 1) 影像学检查示合并腰椎失稳 、 腰椎滑脱 、高髂嵴;(2) 既往脊柱手术史;(3) 合 并马尾综合征;(4) 合并心 、肺 、脑血管基础疾 病 ;合并精神疾病及其他不适合手术治疗的疾病。
1.2 一般资料
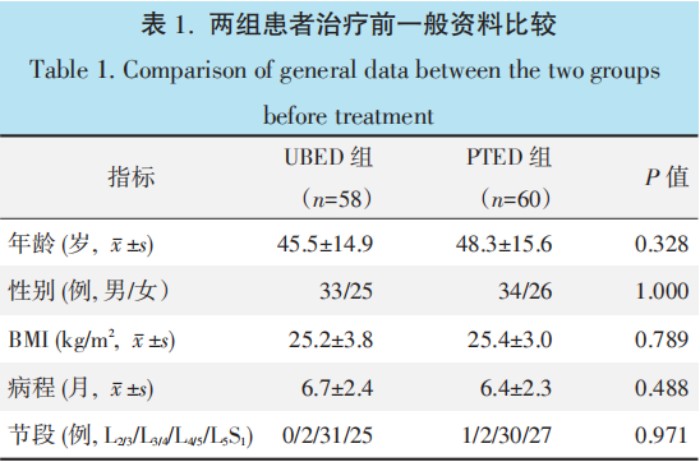
回顾分析 2021 年 1 月—2021 年 12 月脊柱内镜 术治疗腰椎间突出患者的临床资料 ,共 118 例患者符 合上述标准 ,纳入本研究 。根据术前医患沟通结果, 58 例采用 UBED 术 ,60 例采用 PTED 术 。两组患者 术前一般资料见表 1,两组在年龄 、性别 、体质指数 (body mass index, BMI)、 病程和累及节段的差异均无 统计学意义 ( P>0.05)。 本研究获医院伦理委员会批 准(伦理审批号: SRY20210316), 所有患者均知情 同意。
1.3 手术方法
UBED 组 [10, 11]: 全身麻醉成功后患者取俯卧 位 , C 形臂 X 线机引导下用体表定位器透视定位, 以目标椎间隙为中心划一横向标志线 ,以左侧椎弓根 内缘连线作为纵向标志线 ,常规消毒铺巾 ,该两线交 点上 、下 1~1.5 cm 各做一横行手术切口 ,上端切口长 5~10 mm,作为观察通道 ,下端切口长 7~12 mm, 作为操作通道。切开皮肤、皮下组织 ,尖刀片切开深 筋膜 ,逐级扩张至椎板骨性表面。术者左手持内镜并 置入观察通道 ,保证水流通畅 ,右手用低温等离子射 频刀头(江苏邦士 ,AC405)清理椎板及黄韧带表面 软组织 ,显露棘突与上位椎板下缘连接处的骨性标 志。依次显露上位椎板下缘、下关节突内侧缘、上关 节突内侧缘及下位椎板上缘 ,应用高速动力磨钻(贵 州梓锐)与椎板咬骨钳去除上位椎板下缘、下关节突 内侧缘及下位椎板上缘的部分骨质 ,切除部分症状侧 黄韧带 。椎管内应用等离子射频刀头(江苏邦士, AC301) 预止血 ,神经拉钩轻柔拉开硬膜囊及神经 根 ,摘除突出的髓核组织 ,找到纤维环破口 ,清除盘 内松散的髓核组织 ,并对纤维环做成形处理。内镜直 视下在操作通道内放硅胶引流管 1 根 , 缝合 1~2 针 ,覆盖无菌敷料 ,结束手术。典型病例见图 1。
PTED 组[12,13]:患者取侧卧位 ,症状侧在上 ,透 视标记侧方进针点 ,常规消毒铺巾 ,局部浸润麻醉过 椎间孔至椎间隙 ;放置导丝至椎间隙水平 ,透视确认 位置 , 以进针点为中 心作长 7~10 mm 切口 ,导向器 逐级扩张 ,放置工作套管后透视确认位置 ;环锯或高 速磨钻去除部分下位椎体上关节突腹侧骨质 ,打开椎 间孔后壁行椎间孔成形 ,沿工作通道放置椎间孔镜, 到达硬膜囊前间隙及行走神经根的腹外侧 ,直接暴露 神经及突出的椎间盘组织 ,进行镜下突出髓核摘除与 神经松解 ,局部用射频(山东英国正版365中文官网器械有限公 司) 对纤维环进行皱缩成形 ;缝合切口 ,未放置引 流 ,无菌敷料包扎。典型病例见图 2。
术后常规神经营养 、脱水 、镇痛治疗 ,UBED 组 引流通常于术后 24 h 后拔除 。建议术后佩戴腰围 1 个月 ,术后 3 个月内避免剧烈活动。
1.4 评价指标
记录围手术期资料 。采用腰痛和腿痛 VAS 评分及 ODI 评分评估临床状态 。行影像检查 ,测量椎管占位率、椎间隙高度、腰椎前凸 Cobb 角。
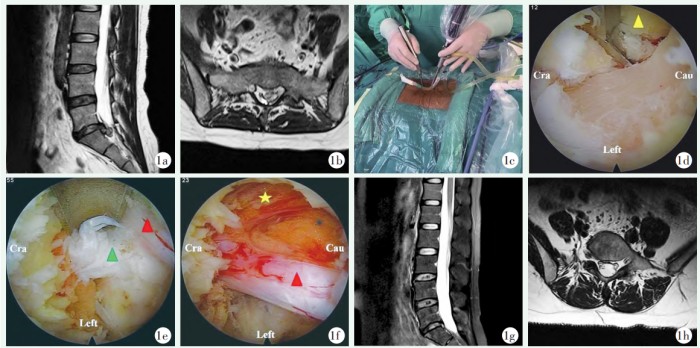
图 1. 患者女性 ,36 岁 ,L5S1 LDH(左侧)。 1a: 术前腰椎矢状位 MRI 示 L5S1 椎间盘左侧突出 ,并挤压左侧 S1 神经根及硬膜 囊 ; 1b: 术前腰椎轴位 MRI 示 L5S1 椎间盘左侧突出 ,并挤压左侧 S1 神经根及硬膜囊 ; 1c: UBED 术中工作通道建立 ; 1d: 椎板 咬骨钳扩大同侧椎板间窗 ; 1e: 术中内镜下左侧 S1 神经根受压状态 ,绿色箭头显示突出髓核组织 ,红色箭头指示左侧 S1 神经 根 ; 1f: 髓核摘除后神经根松弛 ,表面血运恢复 ,红色箭头为左侧 S1 神经根 ,黄色星号为硬膜囊 ; 1g, 1h: 术后腰椎 MRI 示硬 膜囊形态基本恢复 ,S1 神经根无受压。
Figure 1. A 36-year-old female suffered from the left L5S1 LDH. 1a: Preoperative sagittal MRI showed left protrusion of the L5S1 interver⁃ tebral disc with compression on the left S1 nerve root and dural sac; 1b: Preoperative axial MRI showed left protrusion of the L5S1 interver⁃ tebral disc with compression on the left S1 nerve root and dural sac; 1c: Intraoperative working channel establishment for UBED; 1d: A rongeur was used to enlarge ipsilateral interlaminal fenestration; 1e: The left S1 nerve root was decompressed under the endoscope during the operation, the green arrow showing the protruding nucleus pulposus tissue, and theredarrow indicating the left S1 nerve root; 1f: After removal of nucleus pulposus, the nerve root relaxed and surface blood flow recoverd, the red arrow indicating the left S1 nerve root, and the yellow asterisk indicating the dural sac; 1g, 1h: Postoperative MRI of lumbar spine showed that the shape of dural sac was basically recovered and S1 nerve root was not compressed.
1.5 统计学方法
采用 SPSS 24.0 统计软件进行分析 。计量资料以
±s 表示 ,符合正态分布时 ,组间比较采用独立样本
t 检验 ,组内时间点间比较采用单因素方差分析 ;资 料不符合正态分布时 ,采用秩和检验。等级资料采用 秩和检验 。计数资料采用 χ2 检验或 Fisher 精 确检 验。 P<0.05 为差异有统计学意义。
2.1 围手术期资料
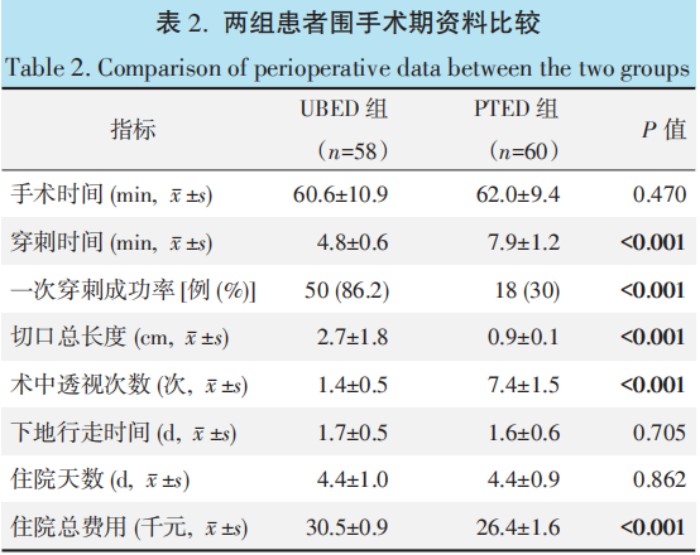
UBED 组和 PTED 组均无神经根损伤及其他并发 症发生 。围手术期资料见表 2,两组在手术时间 、住 院时间 、下地行走时间的差异均无统计学意义( P> 0.05), UBED 组一次穿刺成功率和透视次数显著优 于 PTED 组( P<0.05), 尽管 UBED 组的切口长度和 治疗费用显著大于 PTED 组( P<0.05)。
2.2 随访结果
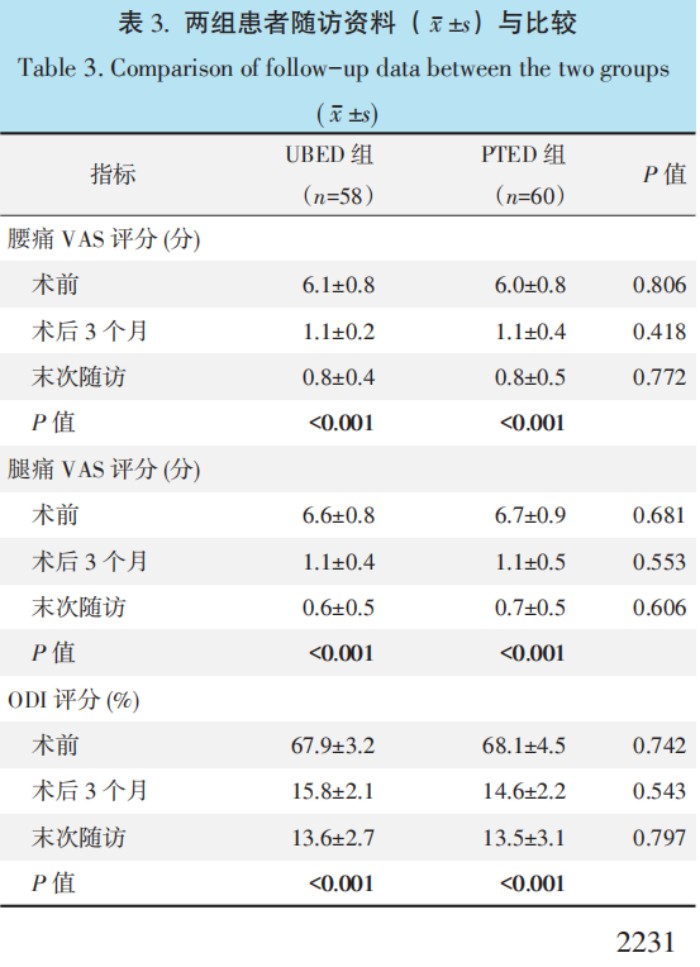
两组患者术后均获随访 , 随访时间为 12~24 个 月 ,平均( 14.1±3.2)个月 。UBED 组随访期间无复 发再突出患者 ,PTED 组有 1 例再突出 ,后再次行 PTED 手术 ,至末次随访无再突出 。两组随访资料见 表 3, 随时间推移 ,两组患者的腰 、腿痛 VAS 评分 及 ODI 评分均显著降低( P<0.05), 相应时间点 ,两 组间上述评分的差异均无统计学意义( P>0.05)。
2.3 影像评估
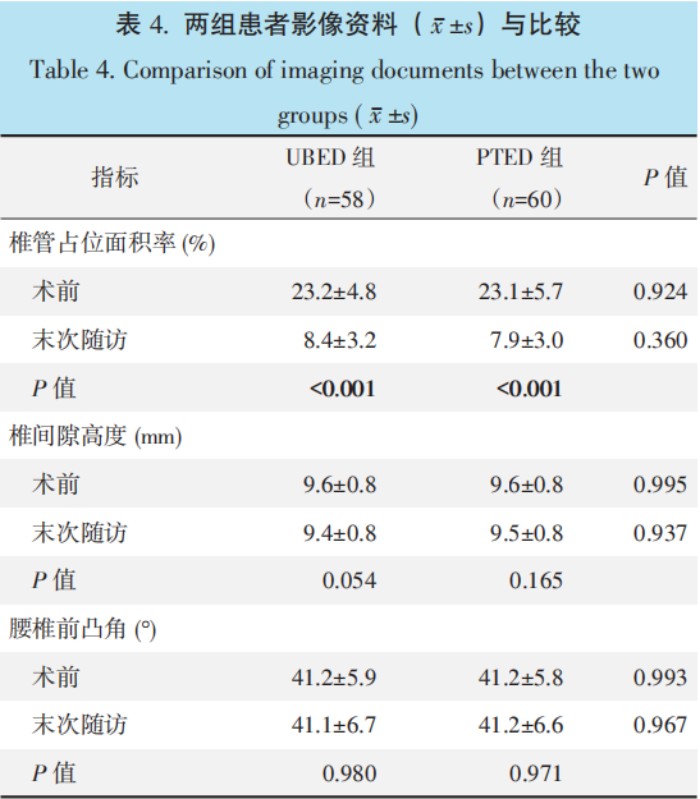
影像评估结果见表 4,两组患者末次随访时病变 节段的椎管占位率均较术前显 著改 善 ( P<0.05), 椎 间隙高度及腰椎前凸角 Cobb 角较术前无明显变化,相同时间点两组间上述影像指标的差异无统计学意义 ( P>0.05)。
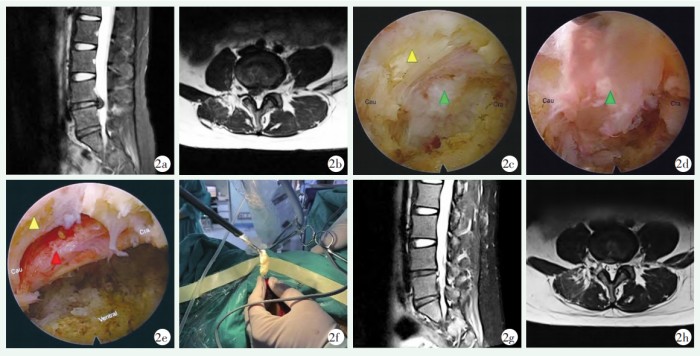
图 2. 患者女性 ,27 岁 ,右侧 L4/5 LDH。2a, 2b: 术前腰椎 MRI 示 L4/5 椎间盘右侧突出 ,并挤压右侧 L5 神经根及硬膜囊 ;2c: PTED 术中内镜下见右侧 L5 神经根受压 ;2d: 术中内镜下髓核钳取出突出髓核组织 ;2e: 术中内镜下见突出髓核摘除后神经根 松弛 ,表面血运恢复 ;2f: 术中镜下取出脱出髓核的外观 ;2g, 2h: 术后腰椎 MRI 示硬膜囊形态基本恢复 ,L5 神经根无受压。
Figure 2. A 27-year-old female suffered from the right L4/5 LDH. 2a, 2b: Preoperative lumbar MRI showed right protrusion of L4/5 interver⁃ tebral disc compressing the right L5 nerve root and dural sac; 2c: PTED endoscopic view of compression of right L5 nerve root; 2d: Intraop⁃ erative endoscopic view of the protruding nucleus pulposus removal by forceps; 2e: Endoscopic view after removal of protruding nucleus pulposus revealed the nerve root relaxed with recovered surface blood flow; 2f: The gross appearance of removed nucleus pulposus; 2g, 2h: Postoperative lumbar MRI showed that the shape of the dural sac was basically recovered, with no compression on the L5 nerve root.
3 讨 论
De Antoni 等[14]在 1996 年首 次报道了 UBE 双通 道技术 ,以提高视觉和操作的灵活性 ,在双通道关节 镜下行椎间盘切除术 ,取得了良好的临床效果。由于 术后疼痛少 ,出血少 ,出院时间早 ,其受欢迎程度越 来越高 ,随着认识的提高 ,腰椎间盘突出患者对内窥 镜手术的期望和需求也逐渐增加[15]。
PTED 是治疗 LDH 临床常用术式 ,有软组织损 伤小 、对脊柱稳定性影响较小 、 快速康复等优 点[16~18]。在临床应用中 ,术者也发现了 PETD 相对于 UBED 的一些不足之处 。对于高髂嵴的 L5S1 椎间盘突 出症患者 ,置入椎间孔镜时通常会受到髂嵴的阻挡, 从而造成操作受限[19,20]。穿刺定位时靶点穿刺需反 复透视 ,医生和患者受到的辐射剂量较大。另外 , 由 于 PETD 操作器械及内镜共享 1 个通道 ,只能使用尺 寸较小的专用器械 ,在对肥厚的黄韧带、钙化椎间盘 及骨性侧隐窝进行减压操作时导致减压效率降低。
UBED 相较于 PTED 有以下优势[1,21]:( 1)具有 独立的内镜观察通道和工作通道 ,双通道位置灵活可 调 ,视野范围大 ,利于合并椎间盘钙化、侧隐窝狭窄 患者的充分减压;(2)器械操作不受硬质通道限制, 可以随意调整方向 ,接近传统开放手术视野;(3)可 使用常规手术器械进行镜下操作 ,提高了减压效率; (4)穿刺定位相对 PTED 简单 ,减少透视次数和辐射 暴露 。UBED 的学习曲线相对 PTED 可能更平缓 ,掌 握 PETD 至少需要 40 个案例的学习曲线 ,而 UBED 至少需要 15 个案例才能达到熟练程度[5]。随着手术 例数的增多及经验的累积 , 手术时间也会相应缩 短[22],本研究 UBED 组与 PTED 组手术时长相当, 但 PTED 穿刺路径需经过骨性结构狭小的椎间孔 ,部 分患者穿刺困难 ,需反复术中透视 ,导致透视次数增 多 ,受到的辐射剂量升高 ,相关研究表明 ,辐射与肿 瘤 、 白 内 障 、 白 血 病 等 相 关 疾 病 发 生 有 一 定 相 关[23]。Merter 等[24] 比较 PELD、UBED 和 MED 3 种
治疗 LDH 的微创方式 ,发现在根据辐射暴露的持续 时 间 和 水 平 方 面 平 均 辐 射 剂 量 面 积 值 PELD> UBED > MED,与本研究相似 ,UBED 穿刺定位相对 简单 ,可以有效减少透视时间 。PTED 相对于 UBED 具有以下优势:( 1)局麻下可操作 ,而 UBED 大多 需要全麻或硬膜外麻醉下操作 [1];(2)局部侵袭性 小 ,椎管内干扰少 ,不需放引流管;(3)住院费用相 对更低等优点[2]。
总之 ,UBED 和 PTED 治疗 LDH 均具有良好的 临床效果 ,UBED 双通道操作更灵活 ,视野范围大, 减压效率高 ,穿刺定位简单可以有效减少透视次数及 辐射 ,但总住院费用相对更高。本研究纳入病例的数 量较少 ,且为回顾性研究 ,仍需更多大样本量、多中 心和长期随访的随机对照研究来进一步验证上述观 点。
参考文献
[ 1] Yuan C, Wen B, Lin H. Clinical analysis of minimally invasive per⁃ cutaneous treatment of severe lumbar disc herniation with UBE two-channel endoscopy and foraminal single-channel endoscopy technique [J] . Oxid Med Cell Longev, 2022, 2022: 9264852. DOI: 10.1155/2022/9264852.
[2] Jiang HW, Chen CD, Zhan BS, et al. Unilateral biportal endoscop⁃ ic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of lumbar disc herniation: a retrospective study [J] . J Orthop SurgRes, 2022, 17 (1) : 30. DOI: 10.1186/s13018-02 2-02929-5.
[3] Yu X, Yue H, Wei H, et al. Comparative study of unilateral bipor⁃ tal endoscopic and traditional open surgery in the treatment of lum⁃ bar disc herniation [J] . Altern Ther Health Med, 2023, 29 (5) : 370-374.
[4] 吕成国, 杨勇, 孙宜保, 等 . 可视环锯椎间孔成形经皮椎间孔镜 椎间盘切除术 [J] . 中国矫形外科杂志, 2024, 32 (4) : 296-302. DOI: 10.3977/j. issn.1005-8478.2024.04.02.
Lv CG, Yang Y, Sun YB, et al. Percutaneous transforaminal endo⁃ scopic discectomy with targeted foraminoplasty by visual trephine [J] . Orthopedic Journal of China, 2024, 32 (4) : 296-302. DOI: 10. 3977/j. issn.1005-8478.2024.04.02.
[5] Li Z, Yang H, Zhang Y, et al. Percutaneous endoscopic transforam⁃ inal discectomy and unilateral biportal endoscopic discectomy for lumbar disc herniation: a comparative analysis of learning curves [J] . Eur Spine J, 2024, 33 (6) : 2154-2165. DOI: 10.1007/s00586- 024-08293-8.
[6] Yuan S, Mei Y, Zang L, et al. Percutaneous transforaminal endo⁃ scopic discectomy for upper lumbar disc herniation versus lower lumbar disc herniation: Clinical outcomes and technical consider⁃ ation [J] . BMC Musculoskelet Disord, 2024, 25(1) : 470. DOI: 10.1 186/s12891-024-07588-7.
[7] Yu Z, Ye C, Alhendi MA, et al. Unilateral biportal endoscopy for the treatment of lumbar disc herniation [J] . J Vis Exp, 2023, 15:
202. DOI: 10.3791/65497.
[8] Wu S, Zhong D, Zhao G, et al. Comparison of clinical outcomes be⁃ tween unilateral biportal endoscopic discectomy and percutaneous endoscopic interlaminar discectomy for migrated lumbar disc herni⁃ ation at lower lumbar spine: a retrospective controlled study [J] . J Orthop SurgRes, 2024, 19 (1) : 21.
[9] Kang MS, Hwang JY, Park SM, et al. Comparison of biportal endo⁃ scopic and microscopic tubular paraspinal approach for foraminal and extraforaminal lumbar disc herniation [J] . J Neurosurg Spine, 2024, 41 (4) : 473-482. DOI: 10.3171/2024.4.SPINE23707.
[ 10] 曹臣, 陈书连, 高延征, 等 . 单侧双通道内镜治疗重度脱垂型腰 椎间盘突出症 [J] . 中国矫形外科杂志, 2022, 30 (3) : 273-276. DOI: 10.3977/j.issn.1005-8478.2022.03.18.
Cao C, Chen SL, Gao YZ, et al, Unilateral biportal endoscopy for far-migrated lumbar intervertebral disc herniation [J] . Orthopedic Journal of China, 2022, 30 (3) : 273-276. DOI: 10.3977/j.issn.1005 -8478.2022.03.18.
[ 11] 郭翔, 徐磊, 赵司顺, 等 . 单侧双通道内镜与通道下腰椎间盘切 除术的比较 [J] . 中国矫形外科杂志, 2023, 31 (13) : 1177-1182. DOI: 10.3977/j. issn.1005-8478.2023.13.05.
Guo X, Xu L, Zhao SS, et al. Unilateral biportal endoscopic discec⁃ tomy versus Quadrant-channel discectomy for single-segment lum⁃ bar disc herniation [J] . Orthopedic Journal of China, 2023, 31 (13) : 1177-1182. DOI: 10.3977/j. issn.1005-8478.2023.13.05.
[ 12] Li T, Yang G, Zhong W, et al. Percutaneous endoscopic transforam⁃ inal vs. interlaminar discectomy for L5-S1 lumbar disc herniation: A retrospective propensity score matching study [J] . J Orthop Surg Res, 2024, 19 (1) : 64. DOI: 10.1186/s13018-024-04543-z.
[ 13] Cheng YP, Cheng XK, Wu H. A comparative study of percutane⁃ ous endoscopic interlaminar discectomy and transforaminal discec⁃ tomy for L5-S1 calcified lumbar disc herniation [J] . BMC Musculo⁃ skeletDisord, 2022, 23 (1) : 244. DOI: 10.1186/s12891-022-0518 6-z.
[ 14] De Antoni DJ, Claro ML, Poehling GG, et al. Translaminar lumbar epidural endoscopy: anatomy, technique, and indications [J] . Ar⁃ throscopy, 1996, 12 (3) : 330-334. DOI: 10.1016/s0749-8063(96)
90069-9.
[ 15] Ozer MI, Demirtas OK. Comparison of lumbar microdiscectomy and unilateral biportal endoscopic discectomy outcomes: a single-
center experience [J] . J Neurosurg Spine, 2023, 40 (3) : 351-358. DOI: 10.3171/2023.10.SPINE23718.
[ 16] Gadjradj PS, Rubinstein SM, Peul WC, et al. Full endoscopic ver⁃
sus open discectomy for sciatica: randomised controlled non-inferi⁃ ority trial [J] . BMJ, 2022, 376: e065846. DOI: 10.1136/bmj-2021- 065846.
[ 17] Chen Z, Zhang L, Dong J, et al. Percutaneous transforaminalendo⁃
scopic discectomy versus microendoscopic discectomy for lumbar disc herniation: two-year results of a randomized controlled trial [J] . Spine, 2020, 45 (8) : 493-503. DOI: 10.1097/BRS.000000000 0003314.
[ 18] Ge R, Liu Z, Huang W. Percutaneous transforaminal endoscopic discectomy is a safer approach for lumbar disc herniation [J] . Am J Transl Res, 2022, 14 (9) : 6359-6367.
[ 19] Wang Z, Chen Z, Wu H, et al. Treatment of high-iliac-crest L5-S1 lumbar disc herniation via a transverse process endoscopic transfo⁃ raminal approach [J] . Clin Neurol Neurosurg, 2020, 197: 106087. DOI: 10.1016/j.clineuro.2020.106087.
[20] Choi KC, Park CK. Percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation: consideration of the relation between the iliac crest and L5-S1 disc [J] . Pain Physician, 2016, 16 (6) : 547- 556.
[21] Hao J, Cheng J, Xue H, et al. Clinical comparison of unilateral bi⁃ portal endoscopic discectomy with percutaneous endoscopic lum⁃ bar discectomy for single L4/5- level lumbar disk herniation [J] . Pain Pract, 2022, 22 (2) : 191-199. DOI: 10.1111/papr.13078.
[22] Xu J, Wang D, Liu J, et al. Learning curve and complications of unilateral biportal endoscopy: Cumulative sum and risk-adjusted cumulative sum analysis [J] . Neurospine, 2022, 19 (3) : 792-804. DOI: 10.14245/ns.2143116.558.
[23] Bosch de Basea Gomez M, Thierry-Chef I, Harbron R, et al. Risk of hematological malignancies from CT radiation exposure in chil⁃ dren, adolescents and young adults [J] . Nat Med, 2023, 29 (12) : 3111-3119. DOI: 10.1038/s41591-023-02620-0.
[24] Merter A, KaraeminogullariO, Shibayama M. Comparison of radia⁃ tion exposure among 3 different endoscopic diskectomy techniques for lumbar disk herniation [J] . World Neurosurg, 2020, 139: e572- e579. DOI: 10.1016/j.wneu.2020.04.079.
(收稿:2024-01-29 修回:2024-11-29)
(同行评议专家:刘凌 ,毛路)
(本文编辑:郭秀婷)
电 话:0538-8161816总部地址:山东省泰安市岱岳区南留街9号
互联网药品信息服务资格证书 证书编号:(鲁)-非经营性-2022-0585
英国正版365官方网站|中文-Made in China 版权所有 ©

